
Dingo
Member
Hello all,
A current claim circulating heavily in right-wing circles on Twitter and frequently in the comments of tweets made by the President, is that Covid-19 deaths are being artificially inflated in the U.S. This inflation is described as all deaths in hospitals being attributed to Covid-19, even traumatic injury deaths (e.g. car crash, murder etc.) The reason for this inflation is given as either financial, as Covid-19 deaths are paid more highly for the hospital than any other; or political in order to extend the lockdown. Obviously the political motivation cannot be debunked, however possibly the financial could be. I will however be focusing on the factual accuracy of the number inflation claims.
Covid-19 Deaths With Underlying Causes/not confirmed by testing
This portion of the claim attests that doctors are being improperly instructed to fill out death certificates as being Covid-19 when underlying or pre-existing conditions are present in a patient. Some statements from doctors are being used to back this claim. For instance, on April 8 2020, Chris Berg of West Dakota Fox posted this interview with Senator Dr. Scott Jensen (R. Minnesota):
Source: https://twitter.com/chrisbergpov/status/1247680994821509121?lang=en
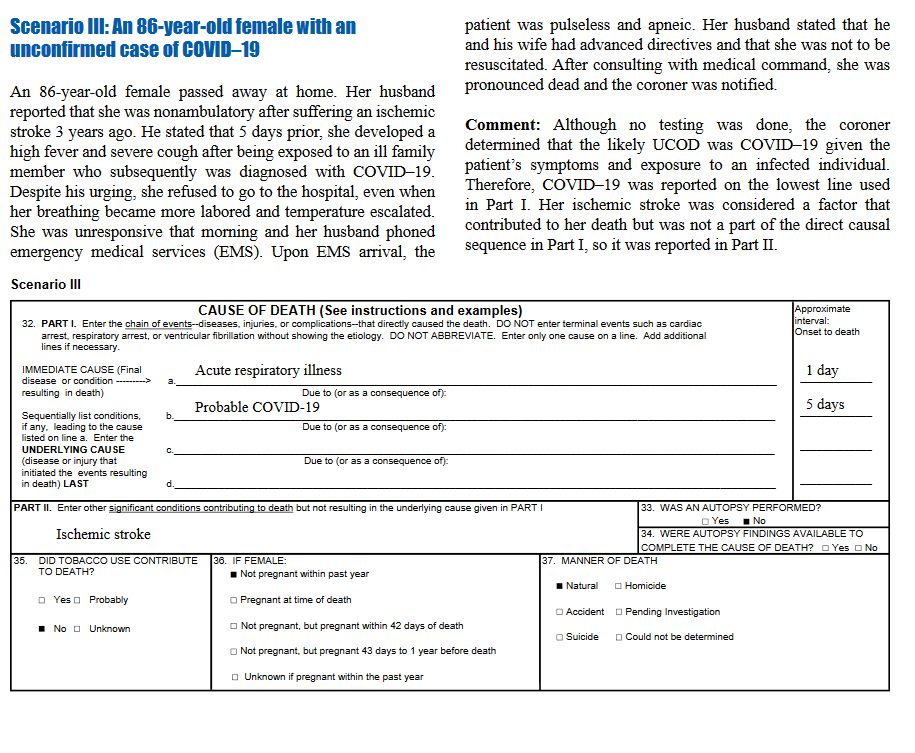
Now the document that he was referring to is the CDC guidelines for certifying deaths due to COVID-19, which was linked in a comment by Chris Berg, and is available from the CDC here. Reading through the CDC guidelines, the scenario talked about by Senator Dr. Jensen is given as scenario III, on page 6 of the document.
The description given by Sen. Dr. Jensen is inaccurate as to the actual content of the document.
The instructions given are for two portions of the death certificate. Part I is:
Here is a screen cap of the example that Sen. Dr. Jensen was referring to:
Now, the claim given by Sen. Dr. Jensen is that this is unprecedented and unusual for determining cause of death and filling out certificates. This is not in line with the Physician's Handbook on Medical Certification of Death, 2003 revision. This states on page 19 that:
Traumatic Deaths Misreported as COVID-19
As for traumatic deaths being misreported, per twitter rumours such as the following:
The common thread in all of these is a lack of verifiable details. All claims are made of 'things that they heard' etc. without names. I have been unable to find any evidence of a traumatic death being misreported. Any assistance in research for this one would be appreciated, but until a specific claim and not just rumours on Twitter are seen, this one can be discarded as simple hearsay and the internet at work.
The first person quoted also claimed the 'Covid deaths get more money' story. I'd appreciate some help if someone wants to give a rundown of how true that claim is.
As this is the first thread I've created here on Metabunk, feedback is of course appreciated.
A current claim circulating heavily in right-wing circles on Twitter and frequently in the comments of tweets made by the President, is that Covid-19 deaths are being artificially inflated in the U.S. This inflation is described as all deaths in hospitals being attributed to Covid-19, even traumatic injury deaths (e.g. car crash, murder etc.) The reason for this inflation is given as either financial, as Covid-19 deaths are paid more highly for the hospital than any other; or political in order to extend the lockdown. Obviously the political motivation cannot be debunked, however possibly the financial could be. I will however be focusing on the factual accuracy of the number inflation claims.
Covid-19 Deaths With Underlying Causes/not confirmed by testing
This portion of the claim attests that doctors are being improperly instructed to fill out death certificates as being Covid-19 when underlying or pre-existing conditions are present in a patient. Some statements from doctors are being used to back this claim. For instance, on April 8 2020, Chris Berg of West Dakota Fox posted this interview with Senator Dr. Scott Jensen (R. Minnesota):
Source: https://twitter.com/chrisbergpov/status/1247680994821509121?lang=en
Senator Dr. Scott Jenson: Well last Friday I received a seven-page document that told me that if I had an 86-year-old patient with pneumonia but was never tested for Covid-19; but some time after she came down with pneumonia we found that she had been exposed to her son, who had no symptoms but later on was diagnosed with Covid-19, that it would be appropriate to diagnose Covid-19 on the death certificate.
Now we don't do that in the middle of an influenza epidemic if someone has pneumonia and I do not have a test for influenza, I do not diagnose influenza on the death certificate, I will say this elderly patient died of pneumonia.
Now the document that he was referring to is the CDC guidelines for certifying deaths due to COVID-19, which was linked in a comment by Chris Berg, and is available from the CDC here. Reading through the CDC guidelines, the scenario talked about by Senator Dr. Jensen is given as scenario III, on page 6 of the document.
The description given by Sen. Dr. Jensen is inaccurate as to the actual content of the document.
The instructions given are for two portions of the death certificate. Part I is:
For Part II:This section on the death certificate is for reporting the sequence of conditions that led directly to death. The immediate cause of death, which is the disease or condition that directly preceded death and is not necessarily the underlying cause of death (UCOD), should be reported on line a. The conditions that led to the immediate cause of death should be reported in a logical sequence in terms of time and etiology below it.
The UCOD, which is “(a) the disease or injury which initiated the train of morbid events leading directly to death or (b) the circumstances of the accident or violence which produced the fatal injury” (7), should be reported on the lowest line used in Part I.
It also notes that:Other significant conditions that contributed to the death, but are not a part of the sequence in Part I, should be reported in Part II. Not all conditions present at the time of death have to be reported—only those conditions that actually contributed to death.
So, it is up to the attending physician, coroner, or medical examiner to determine whether or not the case was probable Covid-19, and this is a valid entry on a death certificate.In cases where a definite diagnosis of COVID–19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty), it is acceptable to report COVID–19 on a death certificate as “probable” or “presumed.” In these instances, certifiers should use their best clinical judgement in determining if a COVID–19 infection was likely. However, please note that testing for COVID–19 should be conducted whenever possible.
Here is a screen cap of the example that Sen. Dr. Jensen was referring to:
Now, the claim given by Sen. Dr. Jensen is that this is unprecedented and unusual for determining cause of death and filling out certificates. This is not in line with the Physician's Handbook on Medical Certification of Death, 2003 revision. This states on page 19 that:
A diagnosis of probable Covid-19 based off of the patient's symptoms and case history is completely appropriate, in line with existing policy, and not an example of artificial inflation of numbers. Snopes.com also provided their own rundown of this claim here and reached much the same conclusion.The cause-of-death information should be the physician’s best medical OPINION. Report each disease, abnormality, injury, or poisoning that the physician believes adversely affected the decedent. A condition can be listed as ‘‘probable’’ if it has not been definitively diagnosed.
Traumatic Deaths Misreported as COVID-19
As for traumatic deaths being misreported, per twitter rumours such as the following:
orAs far as covid patients dying I will bet the 65,000 Cuomo says their were in New York is probably only 20,000. Remember people die of natural cause and cancer car accidents murder gunshots but by some miracle no one died of anything but covid! Why money each covid worth money
(Tweets not linked directly as these people are not public figures and were found via twitter search)Yes there is a awakening. Covid death numbers are inflated. I had a friend whose son committed suicide and death certificate said cause by covid. She has tried to get it changed but hospital says they were ordered to put all deaths as covid that is fraud. Hoax? Yes!!
The common thread in all of these is a lack of verifiable details. All claims are made of 'things that they heard' etc. without names. I have been unable to find any evidence of a traumatic death being misreported. Any assistance in research for this one would be appreciated, but until a specific claim and not just rumours on Twitter are seen, this one can be discarded as simple hearsay and the internet at work.
The first person quoted also claimed the 'Covid deaths get more money' story. I'd appreciate some help if someone wants to give a rundown of how true that claim is.
As this is the first thread I've created here on Metabunk, feedback is of course appreciated.
") if it contained data that would further prove your point, i'm going to guess that you would have provided it.
if it contained data that would further prove your point, i'm going to guess that you would have provided it.