EDIT: I replaced the graphic with an updated version that now also includes the UK
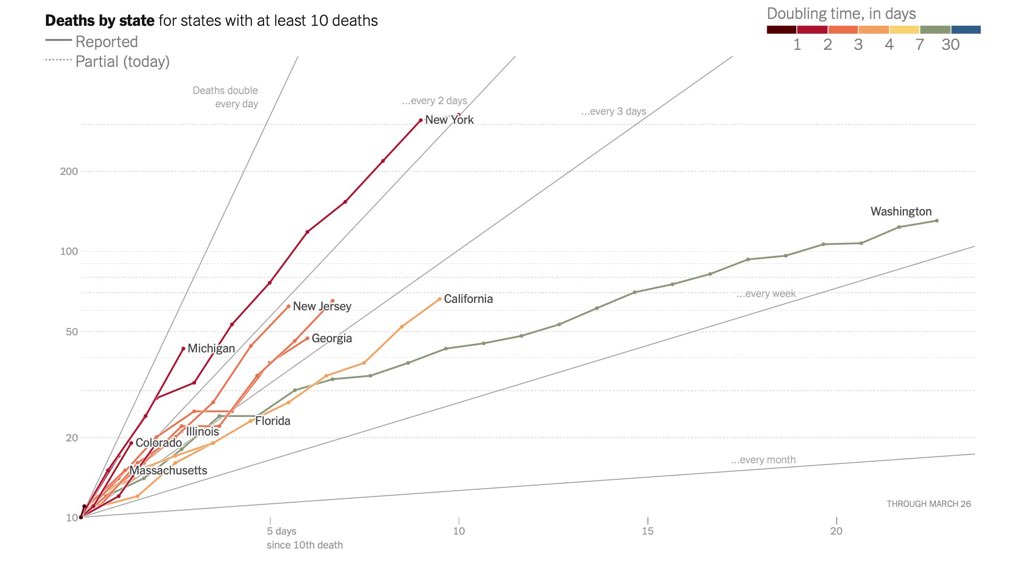
I did the same just now, and came up with my own plot.
The following algorith applies:
- I compute the total number of cases per 1 million people population since the day when a sustained outbreak became visible - i.e. I exclude individual cases caused by people returning early from China that were immediately contained and did not spread. This goes on my x-axis
- I compute the number of new cases in the last 7 days per 1 million people population - that goes on my y-axis
- Both axes are logarithmic.
- For each country, I start plotting on the day it first exceeded 5 cases per 1 million population
- Note that my last data point for each country represent the 29th of March - i.e. today - for which data of course is incomplete
I chose Italy and USA because of prominence, Germany because that's where I live, South Korea as a reliable country known to have gotten a handle on the situation, Iceland because I think I read that they are testing more thoroughly than anyone, Switzerland because I notice they have as many cases as Italy per 1 mio but no one talks about it, Austria just so, Australia because it's in the southern hemisphere.
You see the trend you are all probably familiar with: All countries follow the same trajectory more or less, with only SK having escaped from it decisively. Italy and perhaps Switzerland seem on the verge of escaping the trend (no more exponential growth).
And then there is an item I label "HS", What is that??
It's the "
Kreis Heinsberg" (car license plates here start with "HS-", hence the label), Germany's westernmost district (or county) and home to both the largest sustained Covid outbreak in Germany and to - me

We had our first reported cases (a married couple, both hospitalized, one on ventilator for a while) on February 25th (Italy had recorded its first cases just four days earlier). That was the last day of the carnival season, and the couple had participated in several large carnival event; the wife also works in a kindergarten. This jump-started the epidemic here.
I have taken data from the Covid-19 Dashboard of the Robert Koch Institut:
https://corona.rki.de/
On top, select "Landkreise" (districts) instead of "Bundesländer" (states). Then select "Kreis Heinsberg" from the list on the left. I took the daily new cases from the graphic on the bottom right, augmented by my knowledge that the first 2 cases were on February 2nd.
It seems HS has escaped the exponential growth at approximately the point where Iceland is now - and they, too, seem on the verge of escaping.
This might be a model for non-urban regions in developed countries: Grow exponentially to 2 cases per 1000 inhabitants before slowing down growth rates for cases.
(Iceland however has suffered only 6 deaths per million so far. HS, at about the same point (~2,800 cases per 1 million on March 16th), had 16 deaths per million - and today we already have 122 deaths per million!
I predict that Iceland will have between 20 and 80 deaths in 12 days (April 10th)!)
The next step now is to monitor resolved cases and deduct them from the number of total cases: Are open cases beginning to decline?

")