deirdre
Closed Account
Starting a thread specifically for how the virus (and hospital/medical resources) are being affected by younger people. The CDC released a report (data as of March 16). I added bold and color for highlight.
https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e2.htm?s_cid=mm6912e2_wExternal Quote:
As of March 16, a total of 4,226 COVID-19 cases had been reported in the United States, with reports increasing to 500 or more cases per day beginning March 14 (Figure 1). Among 2,449 patients with known age, 6% were aged ≥85, 25% were aged 65–84 years, 18% each were aged 55–64 years and 45–54 years, and 29% were aged 20–44 years (Figure 2). Only 5% of cases occurred in persons aged 0–19 years.
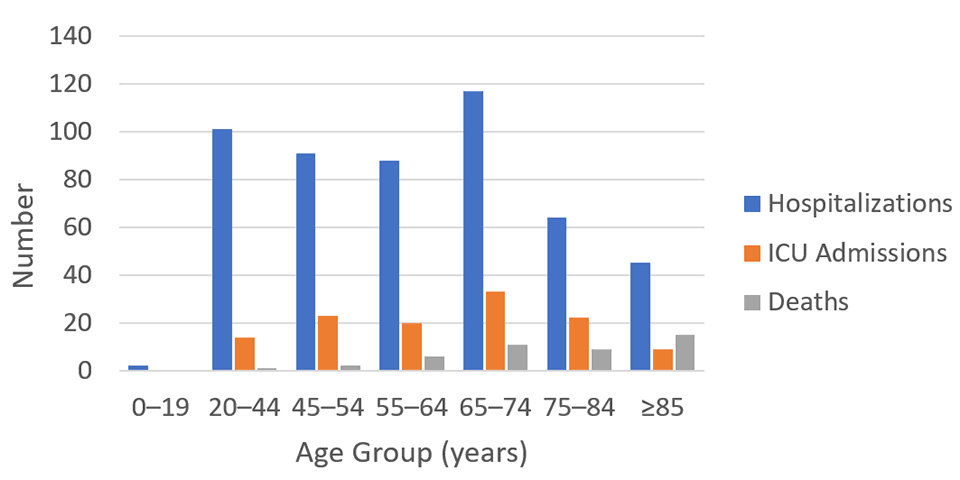
Among 508 (12%) patients known to have been hospitalized, 9% were aged ≥85 years, 26% were aged 65–84 years, 17% were aged 55–64 years, 18% were 45–54 years, and 20% were aged 20–44 years. Less than 1% of hospitalizations were among persons aged ≤19 years (Figure 2). The percentage of persons hospitalized increased with age, from 2%–3% among persons aged ≤9 years, to ≥31% among adults aged ≥85 years. (Table).
Among 121 patients known to have been admitted to an ICU, 7% of cases were reported among adults ≥85 years, 46% among adults aged 65–84 years, 36% among adults aged 45–64 years, and 12% among adults aged 20–44 years (Figure 2). No ICU admissions were reported among persons aged ≤19 years. Percentages of ICU admissions were lowest among adults aged 20–44 years (2%–4%) and highest among adults aged 75–84 years (11%–31%) (Table).
")