This was a handful of GRU agents from Unit 29155 of assassins and saboteurs, led by Col. Ivan Terentiev, who was awarded $1000 for an "acoustic weapon."
"synchronous" means "at the same time". However, the attack occurred after they had left, so it was not synchronous. They were not at the scene.
The claim is, "they traveled back to Russia on the day before one of many claimed 'attacks' on the same continent", and, given that these guys travel a lot and there are a lot of such attacks reported, this feels like it could be random, and isn't even synchronous.
It's a very rare syndrome. Roman Dobrokhotov said it's one in a million, and that if you google "Minor's syndrome" in Russian, the top search result is The Kirov Military Medical Academy.
Again, context! Why is this the top search result, perhaps because of conspiracy theories? What causes thecsyndrome normally, perhaps loud noises like gun fire? The German army operates a hospital specializing in tropucal diseases, but it doesn't mean they cause them.
What percentage of AHI sufferers have actually been diagnosed with Minor's?
I'm not the original poster, but I've been following this story. The Insider article doesn't mention anything about a $1000 reward, but it does mention a reward:
And The Insider, 60 Minutes and Der Spiegel can now reveal, senior members of Unit 29155 were themselves tasked with, and rewarded for, successfully testing “non-lethal acoustic weapons.”
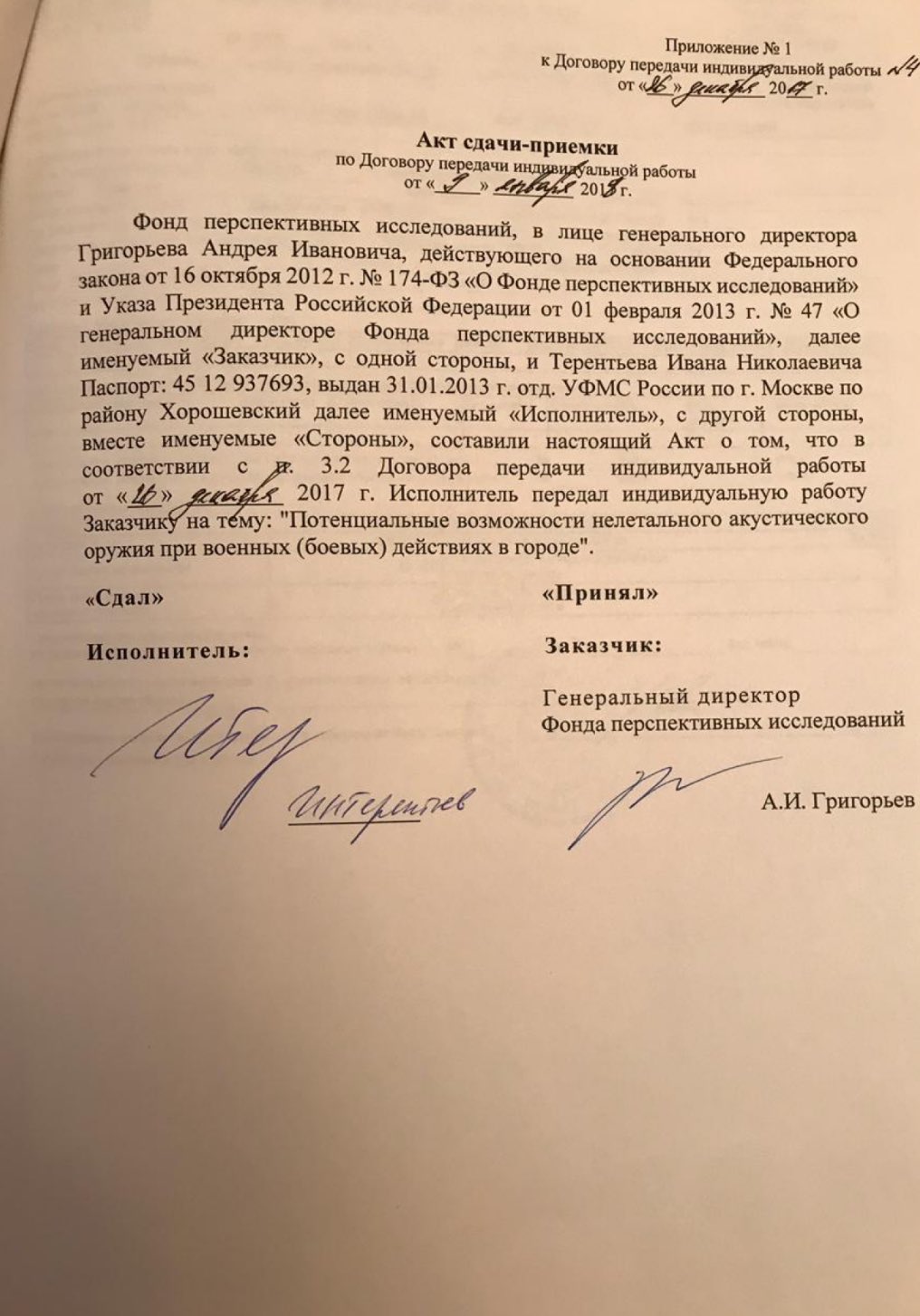
One of the Insider editors posted a photo of an allegedly secret Russian document to support the claim:
The relevant bit of the translation (per Google Translate):
The Contractor [Terentiev] handed over an individual work to the Customer on the topic: “Potential capabilities of non-lethal acoustic weapons during military (combat) operations in the city.”
Regarding the hypothetical existence of microwave weapons related to AHIs, here's my attempt to summarize the arguments:
Pros (i.e. such weapons do exist):
Intermediate range microwave-based antipersonnel weapons in the form of so-called "pain rays" are a well-known capability with public demonstrations dating to at least 2008:
A 60-Minutes episode from 2008 shows a demonstration of the weapon: Source: https://www.youtube.com/watch?v=J1w4g2vr7B4
This video is less than 90 seconds long and shows the reporter failing to tolerate the "pain ray" at about 1:00.
A military demonstration from 2012 gives a larger scale example where the weapon is deployed against a crowd of volunteers at about 0:48. The crowd immediately runs out of the beam: Source: https://www.youtube.com/watch?v=kzG4oEutPbA&t=48s
These weapons use wavelengths that only penetrate human skin far enough to reach superficial nerves, but creating a similar weapon that causes nondeterministic traumatic brain injuries does not seem farfetched.
Cons (i.e. such weapons do not exist):
No such weapon is publicly known to have been captured nor is publicly known to be in inventory.
Publicly known microwave antipersonnel weapons are large (truck sized). Without a captured weapon or better data about the exact circumstances of alleged injuries, it's difficult to assess whether such weapons could reasonably be miniaturized or emplaced.
I'm not the original poster, but I've been following this story. The Insider article doesn't mention anything about a $1000 reward, but it does mention a reward:
And The Insider, 60 Minutes and Der Spiegel can now reveal, senior members of Unit 29155 were themselves tasked with, and rewarded for, successfully testing “non-lethal acoustic weapons.”
One of the Insider editors posted a photo of an allegedly secret Russian document to support the claim:
There's an article at The Skeptical Enquirer which addresses the recent claims about "Havana syndrome", i.e. this is about Unit 29155 and the document you posted:
Pelley points the finger of blame at a special Russian military unit known as 29155. It was disclosed that a Russian journalist had found a document where one the unit’s officers had been paid for his work on “nonlethal acoustic weapons.” Firstly, acoustic weapons involve sound, not microwaves, which is supposedly the weapon involved. Second, acoustic weapons known as long-range acoustical devices (LRADs) or sound cannons have been used by governments for decades to break up riots and political demonstrations. As early as 1989, the U.S. military blasted loud Guns N’ Roses music to get Panamanian dictator Manuel Noriega to surrender (Myre 2017). Commercial container ships have used LRADs for some time to keep pirates at bay. That a Russian military officer worked on an acoustic weapon should come as no surprise. Such weapons, while in use, are very limited because they do not work well due to the laws of physics as the sound wave quickly disperses and would bounce off the outer walls of buildings. It is worth remembering that many of the attacks in Cuba were reported to have taken place inside large hotels. To target an individual inside such a structure with a beam of sound, as has been claimed, is the stuff of science fiction.
The hypothesis of an outbreak of Mass Psychogenic Illness (MPI) relies on a condition which is firmly known to exist, which greatly beats the hypothesis of sonic/microwaves weapons on the prior probability, because even the possibility of making a device which does brain harm at distance while at the same time being undetectable is very much doubtful.
Moreover MPI is supported by the evidence we have, because the reported symptoms are exactly what one would expect from an outbreak of MPI, which in turn neatly explains the whole event. Instead, undetectable sonic/microwave weapons require the added assumption that, when used, they will actually cause the reported symptoms (they could exist buit cause different symptoms, ie., skin rashes or running nose or whatever) which is by no means an estabilished thing, and propping up an hypothesis with an added assumption automatically decreses the probability of it being true (if you prefer Occam, it's 'a multiplication of entities').
I'd say the overall probability ratio of MPI vs. sonic/microwaves weapons is at least 2000 to 1 (1000:1 for the prior probability, and I'm being quite generous here, and another 2:1 for the unproved assumption needed to prop up the sonic/microwaves weapons hypothesis, halving the probabilty being the bare minimum when an unproved assumption is being added). In percentage, it's about 99.95% vs. 0.05%
Firstly, acoustic weapons involve sound, not microwaves, which is supposedly the weapon involved.
I agree that it's extremely unlikely that a sound-based weapon (LRAD) is even remotely related to any of these cases in any way. There's no plausible way to use a LRAD in a clandestine manner.
However, the SI author missed the part of the Insider article in which the author states that the Russian term "acoustic weapons" is conventionally also used to refer to EM-based weapons:
Among this investigation’s core findings is the fact that senior members of the unit received awards and political promotions for work related to the development of “non-lethal acoustic weapons,” a term used in Russian military-scientific literature to describe both sound- and radiofrequency-based directed energy devices, as both would result in acoustic artifacts in the victim’s brain.
One could argue that he's making this up to add plausibility, but as the Weiss is a fluent Russian speaker with a high level of expertise in Russian military and intelligence topics, I'm inclined to trust his explanation. I heard Weiss interviewed yesterday about this article and he stated that he doesn't think it proves the EM hypothesis; his argument is that the number of coincidences involved by way of intersection with the GRU demands additional explanation from the US Director of National Intelligence (which I would say we are unlikely to get).
As to the MPI hypothesis: MPI plus other causes could both be true; i.e. some large percentage of cases could have non-malicious explanations while a few could be malicious. I don't have a rival probability estimate but 2000:1 seems off to me. @Mauro are you saying that you think 1 in 2000 cases might be malicious, or that there's a 1 in 2000 chance that any case is malicious?
My initial guess would be something like: 90% confidence that >90% of reports have non-malicious causes. Of the remaining 10%, I don't have a sense of how to assign probabilities.
I don't have a rival probability estimate but 2000:1 seems off to me. @Mauro are you saying that you think 1 in 2000 cases might be malicious, or that there's a 1 in 2000 chance that any case is malicious?
What I said is I estimate the odds are at least a 1:2000 that the cases are 'malicious' (sonic/microwave weapon) vs. being non-malicious (caused by Mass Psychogenic Illness). In other words: should I being offered a bet on 'malicious' or 'non-malicious' I'd bet 'non-malicious', even at 2000:1 (that is to say: up to betting 20$ against a payoff of 1 cent. If the truth is 'malicious' I lose my 20$, if the truith is 'non-malicious' I end up with 20.01$ ).
My initial guess would be something like: 90% confidence that >90% of reports have non-malicious causes. Of the remaining 10%, I don't have a sense of how to assign probabilities.
Then you should at most accept a bet at 9:1 (let's assume the remaining 10% cases are in fact malicious): at most 9 cents, with a payoff, in case you win, of 1 cent (as in the previous example).
As @Mendel is always very fond to remind us, I'm "not assigning probabilities, just making up numbers", which is mildly annoying to hear, but which introduces the second part of my answer to @Bird. 'Initial guesses' are not bad at all, however they can often be improved. This is why I just avoided to only 'make up numbers', instead I showed Mass Psychogenic Illness has a prior probability of existing of about ~100%, while "sonic/microwave weapons which can do harm at distance while at the same time being undetectable" surely have a much lower probability than that. My 1:1000 probability estimate is a made-up number, of course, but everybody is free to make up its own number and then use it the same way I did. It's the method which matters, not the exact numbers one puts in, and the conclusion is always the same: Mass Psychogenic Illness has a higher prior probability than "sonic/microwave weapons which can do harm at distance while at the same time being undetectable".
The second division by 2 is a given: every time an additional hypothesis is added, and we have no idea if the hypothesis is true or false, it could be 50% true or 50% false, so we need to halve the probabilities (or double the odds). You can think of this as Occam's razor put in a mathematical form. Then of course, should we know anything about the effects of "sonic/microwave weapons which can do harm at distance while at the same time being undetectable", this factor could be refined, in a sens or in the other (but we don't even know if those weapons can possibly exist, it's hard to know something about their effects).
Just to reiterate! The most important thing is the method one uses to try to sort true from false: compare (I stress it: compare!) the odds of two different hypothesis, starting from the prior odds and then adding in the evidence, which means: how much well the 1st hypothesis explains the evidence, compared to the 2nd hypothesis? The exact numbers itself do not matter much, put in yours (honestly) and make your own estimations.
And now I have a question for @Mendel: honestly, how many $ would you dare to bet on Havana Syndrome being caused by Mass Psychogenic Illness vs. sonic/microwaves weapons, with the bet paying 1 cent if Mass Psychogenic Illness is the true answer (you lose your $ if the true answer is 'weapons', you gain 1 cent + your dollars back if the true answer is 'Mass Psychogenic")?
He knows that, that's why he framed them as a "guess".
Would you have preferred he just said "most" rather than "90%"? You couldn't use the "making up numbers" criticism in that case - so what would you use instead? "What do you mean by 'most'?" could be your line of attack. And then you'd force him into revealing a percentage. And then you could finish him off with "you're making up numbers". Another great heroic victory for Mendel!
It seems like you're deliberately trying to misinterpret what is being said.
It's the method which matters, not the exact numbers one puts in, and the conclusion is always the same: Mass Psychogenic Illness has a higher prior probability than "sonic/microwave weapons which can do harm at distance while at the same time being undetectable".
So don't use numbers! They're not required to arrive at this conclusion.
And if you do use numbers, call them your "personal confidence", instead of labeling them a probability that hasn't and won't be measured.
Btw., 90% confidence that 90% are true amounts to a bet value of 81%, not 9:1.
If you did scientific guesses, you'd give uncertainty ranges, but you don't. Could it be 1:500 or 1:4000? If yes, why imply an accuracy inherent in 1:2000 that isn't there?
Because even the uncertainty of any such estimate is unquantifiable, I'm less inclined to bet on this than I usually am. But I'll happily sacrifice $0.01 to have your $20 placed in escrow indefinitely until you figure out a way to decide that bet.
He knows that, that's why he framed them as a "guess".
Would you have preferred he just said "most" rather than "90%"? You couldn't use the "making up numbers" criticism in that case - so what would you use instead? "What do you mean by most?" could be your line of attack. And then you'd force him into revealing a percentage. And then you could finish him off with "you're making up numbers". Another great heroic victory for Mendel!
It seems like you're deliberately trying to misinterpret what is being said.
So don't use numbers! They're not required to arrive at this conclusion.
And if you do use numbers, call them your "personal confidence", instead of labeling them a probability that hasn't and won't be measured.
Probably not, in this case, but what usually happens when people start applying numbers to a problem is that it becomes more rigorous, tractable and solvable.
If you did scientific guesses, you'd give uncertainty ranges, but you don't. Could it be 1:500 or 1:4000? If yes, why imply an accuracy inhetent in 1:2000 that isn't there?
But I did give an un uncertainty range: I said 'at least 2000' (minus 0, plus infinity). This is a fortiori reasoning: using the most unbalanced number I can come up skewed in favor of the hypothesis I'd like to reject (this is another important part of the method). I cannot honestly think there's an odd of more than 1:1000 that an undetectable sonic/microwave weapon can physically exist (but you could well think the odds are 1:500 or even 1:10 or even higher, just be honest with yourself when you write down your number!), indeed I think the actual odds are much more lower, 1 in millions or billions, so I was very generous to the sonic/microwave weapons hypothesis. Your mileage may vary, the conclusion probably won't.
Because even the uncertainty of any such estimate is unquantifiable, I'm less inclined to bet on this than I usually am. But I'll happily sacrifice $0.01 to have your $20 placed in escrow indefinitely until you figure out a way to decide that bet.
My 20$ (well, Euros, in fact) have been deposited in the top drawer of my desk, ready to be claimed! But I'll let you figure out a way to earn them, it would be too much of a hassle for me to do it for a reward of 1 cent
The Insider editor Timur Olevsky says that the Havana syndrome is "Minor's syndrome," or Superior canal dehiscence syndrome. It sounds like what the woman had in Tbilisi.
I think cranioplasty (or craniectomy) is very unlikely here;
(1) small size of incision (2) location (3) the patient looks far too well. Awake, little bruising or swelling. Staples indicate that the op. was done in approx. the past week or so, and she's got too much hair to have had post-trauma neurosurgery or cranioplasty IMHO.
I was wrong about this, in implying it was unlikely that the woman had had a craniotomy. Looked further into the subject; the incision shown is consistent with a small craniotomy to treat superior canal dehiscence syndrome (SCDS). The minimal pre-op shaving is also unproblematic.
Looks like things learned in one context might be different in another...
On realising my errors, like any other Metabunker I smiled to myself, happy that I could put the record straight
@Agent K's observation that SCDS resembles the symptoms of the US woman in Tbilisi is supported by the photos, which may be of someone who has had surgical SCDS repair via a small middle fossa craniotomy.
The claim that the patient had two metal plates inserted into her skull remains sensationalist; the surgeon may have used already-mentioned max-fax mini-plates to fix the returned bone but not a plate to replace part of the skull.
Actually I had real trouble visualising the approach used in SCDS repair, these illustrations helped:
1st illustration from
"Superior semicircular canal dehiscence syndrome", W.L. Bi, R. Brewster, D. Poe et al. 2017, Journal of Neurosurgery 127 (6). Abstract only viewable without payment at this link, https://thejns.org/view/journals/j-neurosurg/127/6/article-p1268.xml.
Other illustrations from Stanford Medicine (Stanford University) Otological Surgery Atlas, Illustrations copyright of Dr. Jackler and Ms. Christine Gralapp, https://otosurgeryatlas.stanford.ed...rgery/superior-semicircular-canal-dehiscence/;
some editing and added labels/ notes by me.
Pics 1 and 2, normal anatomy.
It might be that the woman in Tbilisi was affected by SCDS (also sometimes called Minor's syndrome, but there was another Minor's syndrome beforehand to do with spinal cord injury, so that term is potentially confusing).
SCDS is caused by a malformation of the temporal bone floor which exposes the upper arch of the superior semicircular canal, not initially by a problem with the semicircular canal itself (although the exposed upper surface of its arch may develop a fistula).
It's hard to conceive, realistically, of any ranged weapon method of any sort that could selectively erode the upper surface of the floor of the temporal bone, but not affect the tiny delicate structures of the middle and inner ear, or the outer surface of the temporal bone (at the sides of the head), the eardrum or the bone surrounding the auditory canal.
Nor does this hypothetical weapon seem to cause bleeding in the brain (shows up well on CT), damage to the dura mater surrounding the brain or visible damage to the surface of the temporal lobe (this would be noticed during surgery for SCDS repair) :
The classic MCF approach allows for a top-down repair of a defect; however, it is criticized for extent of temporal lobe retraction
-i.e. the temporal lobe is seen and moved during the procedure;
"Outcomes after Mini-Craniotomy Middle Fossa Approach Combined with Mastoidectomy for Lateral Skull Base Defects",
Walia, A., Lander, D., Durakovic, N., Shew, M., Wick, C.C., Herzog, J., American Journal of Otolaryngology 2021 Jan-Feb; 42(1) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8048087/ (also mentions the dura mater IIRC).
I guess several convergent particle beams could theoretically do this for a perfectly still target if the operator already had head CT/ MRI scans of the target. It would be a huge surgical breakthrough!
However, the "targeted" bone, whether vaporised, liquified or fragmented would have to go somewhere.
The aetiology of SCDS is disputed; Minor himself believes it is primarily congenital (or at least the underlying cause is, a thin area of temporal bone floor):
Based on the results of a large temporal bone study at Johns Hopkins, we believe SCDS is primarily a congenital phenomenon.
In as many as one quarter of cases, however, another inciting injury such as a traumatic head injury or Valsalva initiates symptoms
...they accept that predisposed people who are asymptomatic but already have a thin area of temporal lobe floor over the superior semicircular canal arch might have that thin area damaged by external factors (or a rapid increase in pressure within the head).
Peng, Ahmed et al. (2014) support this, finding SCDS in two patients who have sustained temporal bone fractures
"Temporal bone fracture causing superior semicircular canal dehiscence", Kevin A Peng, K.A., Ahmed, S., Yang I., Gopen, Q., Case Reports in Otolaryngology, 10 September 2014 https://pubmed.ncbi.nlm.nih.gov/25295207/,
although the mechanism is different: Fractures that extended through "normal" temporal bone over the semicircular canal.
Karen F Watters, John J Rosowski, Todd Sauter, Daniel J Lee (2006) describe
"Superior semicircular canal dehiscence presenting as postpartum vertigo" in Otology & Neurotology, 27 (6). https://pubmed.ncbi.nlm.nih.gov/16936563/
With the exception of the two Peng, Ahmed et al. (2014) patients with their traumatic, extended fractures, it seems that SCDS affects people who have an underlying susceptibility. In a minority of cases symptoms come on rapidly after an identified precipitating event (traumatic head injury, receiving the Valsalva manoeuvre, childbirth) but all those patients have an unusually thin layer of bone over the superior canal beforehand.
Although one of the symptoms of SCDS is hearing loud noises, I haven't found any evidence that it is caused by loud noises.
This underlying predisposition to SCDS may be much more common than the rare diagnosis of SCDS suggests,
According to current research, in approximately 2.5% of the general population the bones of the head develop to only 60–70% of their normal thickness in the months following birth. This genetic predisposition may explain why the section of temporal bone separating the superior semicircular canal from the cranial cavity, normally 0.8 mm thick, shows a thickness of only 0.5 mm, making it more fragile and susceptible to damage through physical head trauma or from slow erosion. An explanation for this erosion of the bone has not yet been found.
[Ward, Carey and Minor (ibid). believe genetic factors are a possibility, but are more confident in stating that the condition is congenital regardless of causation.]
It must be possible that the Tbilisi "victim" has suffered SCDS, and has associated its rapid onset with concerns surrounding "Havana Syndrome".
On balance, it must be extremely unlikely that anyone has developed a weapon that can induce SCDS in someone without a predisposition. The weapon would have to be capable of "stealing" a specific layer of bone, which vanishes without trace, from inside the skull, after the beam (or whatever) has travelled through skin, muscle and the temporal bone at the side of the skull, again without leaving any traces or injury, and apparently without damaging any other structures at all (excepting possibly the upper arch of the superior semicircular canal).
In people with a pre-existing temporal bone floor weakness, it seems a variety of physical stressors (childbirth, Valsalva, head trauma) can cause SCDS; more often the appearance of symptoms seems unrelated to memorable health / life events.
I'm not sure it makes sense to develop, and illegally use, a weapon that might injure 2.5% of possible targets when their susceptibility isn't known, even if such a weapon is possible.
Why risk a dependable FSB asset, and perhaps unmask experimental weapons technology, in an attempt to hurt the wife of a member of embassy staff, when she has a 97.5% chance of being invulnerable?
So while the Tbilisi woman might have had sudden-onset SCDS, I doubt very much that this was deliberately caused, or is part of "Havana Syndrome".
I think there's some confusion over what "true" and "false" imply regarding these cases. The phrasing @Bird used was "90% confidence that >90% of reports have non-malicious causes. Of the remaining 10%, I don't have a sense of how to assign probabilities." I'm not sure how @Mendel maps ">90% of reports have non-malicious causes" onto "true", as it sounds more like a "false" to me, accepting the null hypothesis. I'm going to ditch "true" and "false", and just use "mundane" (endogenous or coincidental) and "malicious" (exogenous and deliberate) instead. The estimate proffered with high confidence is that at least 90% are mundane.
But now you're both making assumptions:
- You're assuming that in the 10% where his confidence is unfounded and he's wrong, >90% of cases are mundane. Which is what was said about the proportions when his confidence is well-founded. In which case there would be no reason to bring confidence into the discussion. But it was, so this assumption seems false.
- Mendel, if taking "true" to mean "mundane" (because it's the >90% thing), is assuming that in the 10% where his confidence is misguided and he's wrong, 100% of cases are "false", that is "malicious". He's imagining Bird ending with "And if I'm wrong, they're all malicious" for this assumption to hold. Do we have any reason to believe that's his view?
- One might suppose a third possibility that Mendel tripped himself up with his use of "true", and continued with an assumption that "And if I'm wrong, none are malicious" would have been expressed instead. That would lead to a final probability of 0.91 for any case to be mundane.
In reality, there's been no "And if I'm wrong ..." statement, so we simply don't know what are the best odds to offer. Bird's view of P(mundane) > 0.81, that's a certainty. However, as he said ">90%", we can't specify an upper bound. Hypothesising he'd said "90%", an upper bound would be P(mundane) < 0.91.
Mendel said: Btw., 90% confidence that 90% are true amounts to a bet value of 81%, not 9:1.
Mauro said: if 90% of cases are 'false' and 10% are true, the odds false/true is 9:1 (90/10)
I think there's some confusion over what "true" and "false" imply regarding these cases....
Here I was not making any assumptions about what 'true' and 'false' mean, it was a general statement about bets: I just remarked that if 90% of cases (of whichever thing) are 'type A' and 10% are 'type B' then the odds radio A:B is 9:1, and thus a 9:1 bet would be fair (= repeating many times the bet will result in an average gain of zero), just that.
Here I was not making any assumptions about what 'true' and 'false' mean, it was a general statement about bets: I just remarked that if 90% of cases (of whichever thing) are 'type A' and 10% are 'type B' then the odds radio A:B is 9:1, and thus a 9:1 bet would be fair (= repeating many times the bet will result in an average gain of zero), just that.
But you're ignoring the 10% of the time where his confidence is misplaced, and he's wrong. That 10% slice could be all 10% type A, or all 10% type B. You'll get very different answers in those two extremes - 0.81 - 0.91, as I said above. We don't know his failure mode, and we can't chose for him; we're in the dark.
Probably not, in this case, but what usually happens when people start applying numbers to a problem is that it becomes more rigorous, tractable and solvable.
That is usually because a suitable mathematical model has been chosen (that does not leave important aspects of the issue out), and then measurements are made as inputs to that model.
Your approach is a cargo-cult version of this, where no suitable model has been introduced, and no quantities have been derived from the real world.
the effects of a weapon need to be detectable, else it doesn't do harm.
but we can make it so that that the weapon cannot be be identified with certainty, perhaps: some poisons, for example.
the weapon itself must be detectable, or its operator would quickly lose it.
but we can posit that the weapon should be concealable - in the case of the Havana syndrome, perhaps inside a small van? and that the agent of the weapon is not easily detected: for example, bullets are easy to detect while carbon monoxide requires special sensors.
We have to posit here that the damaging agent is undetectable by the counter-intelligence equipment typically installed in US embassies in communist states.
(or were the AHI "attacks" all away from the embassies?)
That is usually because a suitable mathematical model has been chosen (that does not leave important aspects of the issue out), and then measurements are made as inputs to that model.
Your approach is a cargo-cult version of this, where no suitable model has been introduced, and no quantities have been derived from the real world.
I fear we're veering off-topic here, so maybe a specific thread about epistemology ("the method used to try to determine what is true and what is false") would be better suited, I'll open one in 'chit-chat'.
the effects of a weapon need to be detectable, else it doesn't do harm.
but we can make it so that that the weapon cannot be be identified with certainty, perhaps: some poisons, for example.
Let me remove some of the vagueness: a weapon which does harm at distance without detectable effects except the harm itself. I try to be as precise as possible when making statements, but I thought "sonic/microwave weapons which can do harm at distance while at the same time being undetectable" was already long enough, without adding also "except the caused harm itself".
About poisons: they would surely be a more probable cause than "sonic/microwave weapons", just they were not part of @Bird's argument, so I did not address them. I just compared "MPI" vs. "sonic/microwave weapon".
the weapon itself must be detectable, or its operator would quickly lose it.
but we can posit that the weapon should be concealable - in the case of the Havana syndrome, perhaps inside a small van? and that the agent of the weapon is not easily detected: for example, bullets are easy to detect while carbon monoxide requires special sensors.
We have to posit here that the damaging agent is undetectable by the counter-intelligence equipment typically installed in US embassies in communist states.
(or were the AHI "attacks" all away from the embassies?)
Indeed, and this is a fundamental part of the 1000:1 odds against sonic/microwave weapons: they would be easy to detect, and they would be very very easy to detect once suspicions about their use is raised. For a comparison, poisons would be much more difficult to detect in the first place, and after a suspicion is raised they would become easier to find, but not as much as sound/microwaves.
There's been an incident where 27 members of a Norwegian ship were exposed to microwave radiation from a US ship for 7 minutes, during a joint exercise. 14 were outside the vessel, and the remainder inside. They developed psychological effects.
"Accidental exposure to electromagnetic fields from the radar of a naval ship: a descriptive study" (attached)
Without the presence of visible burns or clear heat sensation, it is considered unlikely that the radiation may cause health effects [8].
The US ship was 90m away, and it caused the malfunction of equipment onboard the Norwegian ship, including the fire alarm, which prompted the crew to ring the US ship and request the radar to be turned off.
The fire alarm made some of the crew rush to the deck, where they got exposed. Some of the exposed felt slight sensation of warmth on the face and arm for a few seconds or minutes. One reported pain in the jaw. None had visible burns or eye symptoms (pain, photophobia or irritation). The physician onboard observed no signs of health problems on anyone, and there were no reports or complaints.
Right after, the Norwegian ship sailed to Russia, as scheduled, where the crew had a weekend off partying, relaxing and sightseeing. Then they went back to sea but the journey was interrupted, as the crew started reporting health problems. It turned out the crew had been writing a symptom diary twice a day. The ship returned and the crew went to the hospital.
The hospital reports describe no signs of disease related to radiation, no burns, cataracts, anaemia, nor dysfunction of testes. There was a meeting with the command, where the crew was informed about the exposure. The crew reported they became more anxious after the meeting. A physician performed an interview with 46 members:
(...) At this time the crew reported problems with headache (43%), fatigue (26%), sweating (20%), pain/burning sensation on the skin (15%), and impaired/disturbed vision (7%). Furthermore, they reported strange feelings in the ear, hearing loss, pain in testicles, nose-bleeding, nausea, and chest discomfort. The onset of symptoms showed considerable variation. One week later the physician wrote in a note that: ‘At the follow-up a week after the original survey, only 1 individual has health problems. The remaining crew has no problems or complaints.’
The crew described they talked a lot about the event and wanted to know about possible health effects, and that they became all worried.
(...) Some of them described that they thought their symptoms developed because they discussed different possible diseases that could be caused by radiation (...)
2 months later, 33 members were still complaining about health problems:
At this time the crew complained about focusing problems, photophobia, headache of various kinds, fatigue and lack of energy. The physician described that they were anxious. Several of the crew were on sick leave and could not work. This was the situation when the crew was referred for examination to the hospital in Bergen at the end of November 2012.
Half of the crew expressed fear their DNA had been damaged, or they became infertile, or were at a higher risk of cancer. But at the hospital, none had eye pathologies, with the exception of 3, who had low tear production and were complaining of dry eyes.
The level of exposure is estimated in the paper:
(...) the radar was a SPY-1D (V), an S-band radar using frequencies3–4 GHz, wavelength 7.5–10 cm [16]. The peak output power of this radar is 6 MW and the average power is 58 kW, which gives a duty cycle of about 1/100. The antenna gain can be calculated from the handbook formula G = 27000/(square of lobe width) [17]. With the lobe width given as 1.7°, the gain will be 9300. With an estimated distance between the ships of 90 m, r, we will have an estimated peak power density (S) of 550 kW/m², according to the formula: S = G × P/4πr², where P is the peak output power. Calculating the peak electric (E) field in the pulse from the formula S = E2/377, this will be about 15 kV/m.
Since the SPY radar has a pencil beam form and has a random search pattern, it is not possible to calculate the exact exposure of the personnel on board the Norwegian ship. If the beam was located at the same spot for some seconds,themean power density then wouldbe of the order of 5.5 kW/m². The rate at which the energy is absorbed by the body when exposed to RF EMF can be measured by the specific absorption rate (SAR). Whole-body exposure at 3–4 GHz gives aSAR = 0.02 W/kgper incoming 1 W/m². For an average of 1 s, with the beam located at the same spot, this will give an exposure of 110 W/kg. The specific absorption (SA) during 1 pulsecan be calculated from SA = S × 0.02 (W/kg)/(W/m²) × t, where t is the pulse length. From data on the net, the pulse length can be up to 50 µs [17], and this would then giveSA = 0.55 J/kg.
In human volunteers undergoing partial-body RF exposure, the warmth sensation can be detected immediately by applying continuous exposure with power density of 270 W/m² at 2450 MHz, giving rise to a spatial peak SAR of 6.6 W/kg.
A report from the U.S. Air Force from 1985 describes similar incidents among a total of 330 people suspected of being‘ over-exposed’. They all described similar symptoms as seen in the present study, but it turned out that only 58 had actually been radar exposed [23, 24]. Such stress reaction following special events has been known for many years, and can also occur in other populations where one fears the health effects of specific exposures [25, 26].
Of course I am just making up numbers! Normally I prefer to phrase things in soft estimates of confidence, e.g. "likely" or "highly likely", but here I was just trying come up with something that felt like it represents my confidence levels in comparison to the 2000:1 estimate given earlier.
We don't have good numbers about the number of reported AHIs; there have been reports ranging from dozens to hundreds.
As to the microwave weapon vs other stuff debate: I intentionally used the term "malicious" when discussing confidence levels, rather than "EM caused". I think the possibility of a microwave weapon that can cause TBIs existing somewhere is reasonable. This is because we already know that microwave weapons exist in other contexts, and we know that RF injuries happen -- I personally have known two people who experienced serious RF injuries, though not from microwave frequencies. But that said, it's highly uncertain whether they could be deployed in a sufficiently clandestine manner to be related to these AHIs.
As to what I think -- I think it's highly likely that:
There are multiple causes of AHIs.
That some of them are common medical problems caused by mundane health problems unrelated to foreign adversaries.
That some of them are related to social contagion (i.e., MPIs).
I think it's possible that a small number are caused by foreign adversaries (with Russia being by far the most likely), with multiple vectors (poisons, microwaves) being possible. When these reports first started coming out, I was pretty sure it would end up being poisons -- Russia has done poisons many times, going back decades. The main reason I think there could be another vector is reporting that claims a small number of cases where imaging is consistent with externally introduced brain trauma and not with poisoning, in subjects with no history of impact TBI. Unfortunately there is no direct public evidence about this; it's merely claimed in news reporting and by victims.
The linked-to paper
["Accidental exposure to electromagnetic fields from the radar of a naval ship: a descriptive study",
Moen, B.E., Møllerløkken, O.J., Bull, N., Oftedal, G., Hansson Mild, K., International Maritime Health 64 (4), 2013]
was an interesting read, thank you @john.phil
Although not overtly stated, the authors effectively ascribe any ill effects to anxiety/ psychosomatic causes:
The crew had clearly less subjective [objective? John J.] health complaints than what we find in a normal population, and the symptoms had evidently disappeared.
These findings are in line with previous studies and overviews of the ‘over-exposure’ episodes, showing that radar exposure only causes health problems when it has led to serious heating of the persons involved...
...Many of the personnel involved were worried about the possibility of long-term health effects. With the current knowledge of radar exposure and health, there is no reason to fear such effects from the radar exposure. They did not seem to have been informed about this present knowledge. Their worries had probably been caused by the lack of information about the radar exposure, as they were thinking the exposure must have been extremely high since they were not properly informed, and since equipment on board the ship was affected
And
...It has been suggested that the symptoms may arise as the persons involved are put in a special stress situation. A report from the U.S. Air Force from 1985 describes similar incidents among a total of 330 people suspected of being ‘over-exposed’. They all described similar symptoms as seen in the present study, but it turned out that only 58 had actually been radar exposed. Such stress reaction following special events has been known for many years, and can also occur in other populations where one fears the health effects of specific exposures
(My emphasis)
The authors make some recommendations for cases of suspected radar over-exposure, including
If there are no signs of heating after an exposure incident, there will be no health problems. This must be stated clearly to the crew and they must also be informed about the knowledge of no risk regarding long-term health effects. However, it might also be important to inform the crew about the high risk of developing subjective health complaints after such an episode, and that this kind of reaction can be quite normal.
(My emphasis)
The authors' advice and conclusions seem pretty straightforward and relatively easy to implement.
Maybe the spread and persistence of "Havana Syndrome" (if we are sceptical of a malevolent targeted cause) would have been more limited had the management of complainants been more in line with the advice given by the Norwegian authors.
E.g., after satisfactory medical examinations, matter-of-fact (but non-judgemental) advice to complainants that their symptoms might be of psychological cause, and it's known that this can happen to people in "special stress situations" (to borrow a phrase from the Norwegian authors) and that the symptoms may persist for some time but will not impact long-term health.
Of course, there may well be understandable reasons why a member of diplomatic staff might not want to accept a "psychological" diagnosis, perhaps even more so if they are in an intelligence role.

")